4.2 Modeling of full breathing cycles
4.2.1 Flow field reverse modeling
Simulation of full breathing cycles requires an integral and highly accurate numerical model that contains all of the relevant components.The components can be grouped into four main parts:human upper respiratory airway,FFR cavity (deadspace),FFR media,and ambient air.Among them,the FFR cavity and FFR media are the key parts in reverse modeling and simulation.Due to the contact pressure when wearing FFR,both the FFR and human face are deformed to some extent.To obtain the precise size and shape of these parts after contact and deformation,two different solutions were taken into consideration:three-dimensional (3D) laser scanning and Computed Tomography scanning.3D laser scanning was not used because it can only record surface data and is unable to recognize the interior geometry of a multilayer object [10-12].For example,the upper respiratory airway cannot be modeled in this way because it has multiple layers.However,CT scanning has the opposite feature,and uses computer-processed X-rays to produce tomographic images (virtual"slices") of specific areas of a scanned object,allowing the user to see inside of the object without dissection;as a result,CT scanning was the method of choice for this work.The size,shape and position of most parts in this model can be easily obtained by CT scanning,except for one important part:the FFR medium.Because the FFR fiber is too thin and low density to block the X-ray beam,it is almost invisible during CT scanning.Ultravist is reported to be a water-soluble contrast medium that is harmless to human skin.It is widely used to differentiate"invisible"parts and make them visible in CT scanning [21].The 3M 8210 N95 FFR was chosen and steeped in Ultravist for a sufficient amount of time so it would become visible during CT scanning.The wetted FFR was then worn normally by the subject and scanned with a headform simultaneously so that each part could be objectively obtained.
The nose clip was removed before CT scanning because it is made of aluminum alloy and a direct CT scanning of this material will generate numerous noise points.Moreover,the FFR became airtight after it had absorbed the Ultravist so that asphyxia could occur during a CT scanning lasting for several minutes.Therefore,a leakage was deliberately maintained above the nose during CT scanning and then was manually sealed during model processing.There is a discrepancy between the CT scanned geometry and the modeled geometry,but that discrepancy is unavoidable in the prevention of asphyxia.The CT scanning was implemented and accompanied by professional medical workers in case of an emergency.The medical images obtained in the Digital Imaging and Communication in Medicine (DICOM) format from CT scanning were transferred into Stereo Lithography (STL) format containing point cloud data,as illustrated in Fig.4-1.

Fig.4-1 Point cloud generation for respiratory airway (yellow),FFR (green) and headform (pink)
Fig.4-1 shows the axial,coronal,sagittal and axonometric views of the respiratory airway (yellow),FFR (green) and headform (pink).Prior to a high-quality mesh generation,each part was partitioned using commercial software (MIMICS 16.0,Materialise,Belgium).Considering that the headform part was closely bonded with the FFR part,it was difficult to directly separate them.A Boolean Operation (minus) was conducted,and the upper respiratory airway model was also separated in this way.Flaws and tiny unnecessary features,such as holes and spikes that can lead to a bad mesh quality,may be generated during CT scanning due to the geometric complexity of the respirator and headform.Therefore,the CAD models were manually smoothed using a reverse modeling software (Geomagic Studio 12.0,Geomagic,Rock Hill,NC,USA).
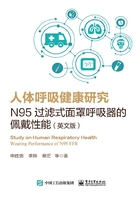
Fig.4-2 shows the variance contours of smoothed CAD models compared to the original point cloud models.The variance in most areas (green area) is less than 0.46 mm.It demonstrates the high fidelity of the three parts of the CAD models.

Fig.4-2 Variance contours of the upper respiratory airway,headform and FFR (Unit:mm)
A cuboid zone (600 mm×600 mm×600 mm) was created and a Boolean Operation was used to segment it into the FFR cavity and surrounding flow field.Prior to the CFD simulation,the pre-processing of the CAD models was implemented and meshes on the four different parts were generated (ICEM CFD 12.0,ANSYS,Canonsburg,PA,USA).Fig.4-3 shows the fluid zone for this simulation,which was divided into four zones:namely surrounding ambient air,FFR media,FFR cavity and upper respiratory airway.Meshes for Zone 1 were generated using mixed elements because of the high fidelity of the headform and large scale of the whole model.The tetrahedron element was used to ensure the mesh quality around the headform.The hexahedron element was used for the rest of Zone 1 to reduce the element number.Using mixed elements to obtain high-quality mesh with acceptable element numbers has been proven feasible in a previous study [22].Meshes of Zones 2,3 and 4 were generated using the tetrahedron element.The final model included 703,200 tetrahedron and 162,000 hexahedron elements after performing a grid independence test.

Fig.4-3 Mesh and boundary condition for CFD simulation:(1) ambient air,(2) FFR media,(3) FFR cavity,(4) upper respiratory airway and (5) the profile of normal respiratory flow rate (L/min) [14] (free stream flows along with the arrows)
4.2.2 CFD simulation of a full breathing cycle
The CFD simulation of a full breathing cycle was implemented using CFD software (FLUENT 12.0,ANSYS,Canonsburg,PA,USA).
(1) For the tidal air flow from respiratory airway to ambient air,no high-pressure source exists which can lead to considerable air compression,and the real breathing procedure is time-dependent;consequently,an unsteady incompressible model was chosen.The RNG (ReNormalization Group) k-εturbulence model was used because it has proven to be an accurate predictor in indoor air simulations [10,23-24].In addition,it has also been used in a simulation of flow through airways [25].
(2) The heat accumulation issue proved challenging because heat exchange among the environment air,deadspace air,FFR material,the different facial layers of muscle,fat and blood are complex.Simulation of heat exchange has been implemented previously to detect leakages while wearing an FFR [10].Research also showed that the use of N95 FFR resulted in non-significant,minimal increases in core temperature,and uncovered facial skin (cheek) temperatures [6].Considering that we primarily focused on the airflow-related cause of FFR discomfort,the heat exchange between air and face was neglected.This simulation assumed that the main source for temperature rise is the high-temperature exhaled airflow,not the face or other sources.
(3) When modeling the air species transport through the FFR,it is assumed that there is no water phase change (water vapor became water liquid or vice versa) and no chemical reaction.Initially,ambient air occupies the whole domain at standard atmospheric pressure.At a temperature of 296.6 K,the standard ambient air composition is calculated to be 0.03%CO2,20.71%O2,1.23%H2O and 78.03%N2,and the exhaled air composition is calculated to be 4.88%CO2,15.61%O2,2.44%H2O and 77.07%N2 [26].
(4) The filter medium of the FFR was assumed to be a porous medium to simulate its resistance to air flow.In the laminar flow through porous media,the pressure drop is proportional to the velocity,and the momentum equation is replaced by Darcy's law [27]

where 1/α is the viscous resistance coefficient.A viscous resistance coefficient,1/α=1.12×1010m-2,was used for the FFR filter medium,based on experiments quantifying the air permeability of the N95 FFRs [28].An effective conductivity in the filter medium was used in the heat conduction equation

whereε,ρf, cfand kfare the porosity,density,specific heat,and thermal conductivity of the FFR filter medium,respectively.
Considering that normal breathing with a low respiratory flow rate matches our problem well,pure nasal breathing was simulated for exhalation and inhalation.Table 4-1 lists the necessary details of the CFD simulation.
Table 4-1 Details of the CFD simulation

A velocity inlet boundary condition was defined on the lowest horizontal cutting plane of the upper respiratory airway so that the exhaled air would be rectified by the airway before entering the deadspace,instead of manually setting the direction of airflow [10,29].The area of the inlet is approximately 509 mm2.The periodic change of exhalation and inhalation was described by an unsteady air velocity or air flow rate [22,30-31].Tidal flow was taken into consideration by giving the velocity inlet a prescribed profile normal to the boundary.Fig.4-3 defined a time-dependent profile of breathing flow rate during one full breathing cycle [14].The time for a full breathing cycle was defined as T.The profile is piecewise linear,and the exhalation duration (3 s) is longer than the inhalation duration (1.8 s).Consequently,the average respiratory rate is 12-13 breaths per minute.The peak exhalation flow rate is 30.54 L/min,and the peak inhalation flow rate is-27.49 L/min.The temperature of exhaled air was set at 307.6 K [32].The nostrils were defined as the interface to connect the upper respiratory airway and FFR deadspace.
The time step size was set at 0.05 s,and each breathing cycle lasted for 4.8 s (i.e.,96 time steps).It took approximately 40 minutes to run the simulation of each breathing cycle.The total duration of the simulation is 80 hours in CPU time and 11,520 time steps (Intel Xeon CPU E5-2680V2 2 processors 2.80×2 GHz,RAM 128 GB).